
all women difference
We understand the importance of feeling goodOur Procedures
Mastopexy (breast lift)
A breast lift is suitable for patients who have sufficient volume in their breasts but the breasts have dropped after pregnancy and breast feeding or with aging. If in a bra you are happy with the volume of your breasts then this may be more suitable than other forms of breast surgery. If your concerns are both lack of volume and the droopiness of the breasts, it may be an augmentation mastopexy (i.e. a breast lift with implants) may be more appropriate. It can also be possible to have a breast lift after removal of implants rather than having new implants.
As with other surgeries there are different techniques and each have its place. A breast reduction operation such as a superior, inferior or superior-medial pedicle techniques can be used but a small amount of tissue still has to be removed. These techniques can be combined with a breast implant if added volume is needed.
Short scar techniques use some gathering and allow the inherent properties of skin to shrink back. There will be a scar around the nipple, and a vertical scar dropping down to the fold under the breast. Depending on how much skin needs to be excised there may or may not need to be a scar in the fold under the breast. This however is kept within the confines of the fold so it is not visible unless you lift your breast to look. We do not use the traditional anchor scar or “Wise pattern” technique.
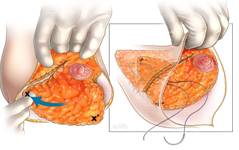
Rotation Mastopexy
This is technique when all the breast volume is maintained and tissue is moved from the bottom and outside of the breast into the empty upper part of the breast. Minimal breast tissue is discarded, only skin. It is a useful technique to use after removal of breast implants to restore the shape of the breast if there is sufficient tissue.



 Rotation mastopexy pre-op and 2 years post-op
Rotation mastopexy pre-op and 2 years post-op



Removal of implants and rotation mastopexy pre-op, 12 months and 3 years post-op
Augmentation Mastopexy
This is when the breast is lifted and implants added for volume. This can be done at the same time, but is often very risky with a high revision rate (35%). If done at the same time it must be conservative with relatively small implants to try and keep the risk of complications down.
There is an option to do the lift first and 3 months later add implants, this is a much safer option, especially if the implants are to be relatively large.

 Before and 2 years after augmentation mastopexy
Before and 2 years after augmentation mastopexy
Implants in an augmentation/mastopexy are usually round implants under the muscle (see augmentation).
Important Issues to consider:
Breast surgery as with all other surgery has its risks and complications. We all need to be prepared for when things do not work out as you hoped and also to work together beforehand to minimise the risks. You need to be fully aware of these issues and know how we will address them so that ultimately you can achieve a good result. In making your decision to go ahead with surgery as well as being aware that your ideal may not be achievable and some compromises may need to be made you need to be able to accept the risks and understand the following issues:
Mammography
Breast lift surgery produces many internal scars. Scar patterns is one of the things that is looked at in mammograms, so if you are 40 years or more it is important that you have a baseline mammogram about 6 months after your operation. Breast surgery does not increase the risk of developing breast cancer.
The Finding of a Lump during surgery
If this occurs the lump is sent away for an immediate pathological examination. If the lump is shown to be a cancer then the operation won’t go any further, and the wounds are closed. To minimise this happening all patients over 40 years are asked to have a pre-operative mammogram. All resected breast tissue is sent away for pathological examination.
Scars
Breast lifts unfortunately leave visible scars on the breast, hence the reason for keeping them short. If you have problems we do have methods to help or can revise them a year later. Nearly all scars will fade out given sufficient time (years) apart from a very few which are true keloids.
Nipple sensation
This will alter. You may become more sensitive, less sensitive or lose sensation altogether. This is unpredictable and each nipple is different, however 75% will return to normal after a couple of years.
Nipple loss
There is a rare risk of nipple loss. This is when the blood supply doesn’t keep up to the nipple. There is a higher risk in smokers and diabetics. If this were to happen you would be able to undergo a nipple reconstruction.
Infection
This is very unusual but if you do get an infection it would be treated with antibiotics.
Lumpiness
This occurs after the operation especially in the denser breasts and takes months to soften up.
Wound Breakdown
This is where the suture line opens up and is slow to heal. It is usually the size of a 5 cent piece, but can be larger and rarely a big crater. These always heal with appropriate dressings and care. Small breakdown areas can occur in association with deep stitches working their way out.
Suture reaction
Occasionally patients can have a local reaction to sutures. Most often this presents as a small pimple/pustule as the suture works its way to the skin surface.
Bleeding
The breast is a gland and so prone to bleeding. If you have a bleed it is nearly always within the first 24 hours after your operation and you need to go back to theatre to have it washed out. A smaller bleed will clot and about 3 weeks later liquefy. This may then be absorbed, or it may discharge spontaneously through the wound.
Unevenness
To get perfectly symmetrical breasts is virtually impossible. If you imagine yourself lying flat with your arms out, as in the operation, your breasts lie very differently to when you are sitting up. Hence getting the shape, position, and size just right is not that easy. Occasionally a minor adjustment is necessary a year later.
Late Changes in Breast Shape
The breasts may grow again late in life, during pregnancy or menopause. They may also drop. It maybe that you would consider secondary surgery later in life. This is especially an important consideration to young patients.
Anaesthetic Complications
Untoward anaesthetic events occur very rarely. They include allergies and anaphylaxis, deep vein thromboses, heart attacks, breathing problems, awareness during the operation. This is why you have your operation in hospital with a qualified anaesthetist and full back up facilities.
The Consultation
On your first appointment you will need to allow about one hour. You will be examined by Dr Ngan and she will discuss with you the different surgical techniques and what is suitable for you. She will also discuss with you what you can do to reduce your risk. You must have a BMI below 30 and have stopped smoking for 3 months. Any chronic medical conditions may need to be addressed before surgery. Dr Ngan will also explain what complications are associated with mastopexy and how we would deal with such an eventuality. This helps you to make a fully informed decision. Any decision to undertake such a surgical procedure should not be taken lightly.
Following your consultation you will be given a written summary of what has been discussed. You will be provided with relevant pamphlets and a written estimate of costs. We encourage you to take this home and study it and write down any questions you may have. If you think that you would like to proceed with surgery then you will be asked to come back for a second appointment. You will see Dr Ngan again and have the opportunity to ask any further questions. You will be measured for surgical bras and do the paperwork. You will also receive a prescription for your post-operative drugs and you may see the Anaesthetist at this visit. We encourage you to ask anything that you are unsure about, no matter how trivial it may seem. You are very welcome to come back just for another chat to further discuss the surgery. This does not mean that you have to go through with it!
The Operation

The surgery takes place in fully-accredited hospital. It is our belief that your safety is paramount concerning both surgery and anaesthesia. You will have the option of having your operation in Melbourne or Geelong. The procedure is performed under general anaesthesia, and a specialist anaesthetist will be giving the anaesthetic. The operation takes about 2 and a half hours and at the end of the procedure local anaesthetic is used to minimize pain. You will be given a prescription for pain relief prior to leaving the hospital. Often patients will opt to stay overnight in the hospital, however if the surgery is performed in the morning, it may be possible to do this as a day stay procedure.
Post-Operative Care
You will be over the worst of the surgery normally in a couple of weeks, but it takes 6 weeks to fully recover. It depends on the demands of your work as to how much time off you will need. We discuss with you the practical issues such as time off work, managing family etc. Due to anaesthetic techniques used, pain relief needed is basically paracetamol and anti-inflammatories plus some stronger tablets ‘just in case’ but these are rarely needed.
The wounds are closed with absorbable stitches and paper tape. You can shower and dry the tapes with a hair dryer. You will be seen one week, and then two weeks post-operatively. You will wear surgical bras day and night for 6 weeks and then day only for 6 weeks to support and gently compress the breasts as they are healing. For any concerns, please call the rooms. Dr Ngan is on call day and night for any urgent concerns. We encourage you to come in and see us if you are worried about anything. Usually we would see you at 6 weeks, 12 weeks, 6 months and 12 months post-operatively.
Exercise
You can go back to low impact exercise such as walking, bike riding, etc, but all high impact exercise and ‘bouncing’ including running should be avoided for 3 months.
Costs
You will receive a written quotation that fully explains the cost of the surgery. This includes post operative care, bras, and dressings. Insurance companies do not usually give you any cover for this type of surgery but it would be worth checking with your health fund as they do occasionally contribute towards the hospital costs.
Disclaimer
All before and after photographs are of patients that have had surgery performed by Dr Ngan or Ms Corduff and have consented to their photographs being used. The photographs have not been altered. Results may vary from individual to individual.