
all women difference
We understand the importance of feeling goodOur Procedures
Breast Augmentation Surgery
Which implant and which operation?
This is the question that causes patients most confusion and concern. We at the Aesthetic Breast Surgery Centre have an approach that individualises both the surgical technique and implant choice to the patient. The most important thing we work together on is your desired outcome in terms of shape and size. We then work through what can reasonably be achieved based on your underlying breast and chest wall shape and size as well as your tissue quality, occupation, exercise requirements etc.
There are many different approaches to the surgery and many different implants available. Each can have an influence on the final outcome and it is the experience of over 20 years in surgery that enables us to work closely with you to pick the right implant and technique. No one technique and no one style of implant will suit everyone. Also a round implant does not always give a round breast, and alternatively an anatomical implant does not always give a tear drop shaped breast!
Cosmetic Tourism - There's no need to travel overseas
Are you considering Breast Surgery overseas because you can't afford to have it done in Australia?
The significantly reduced cost of surgical procedure overseas is what attracts many to what we call 'Cosmetic Tourism'. For the same reduced cost, you can have your surgery in Australia where you can be fully confident that you are receiving the highest standard of medical care.
Click Here To Find Out More...
Breast Implants:
Shape vs Volume
When breast augmentation first came into being, the only option available was to increase the volume of the breast without giving consideration to the shape of the breast. Our approach is to firstly consider your desired breast shape. Very broadly we have described 3 different shapes:
Texan look


This shape is characterised by the upper part of the breast being filled in a gradual slope towards the collar bone. This can vary from subtle to a very full breast.


Gold Coast look


This is characterised by a step to the upper part of the breast from the chest wall. The upper part of the breast is noticibly rounded as opposed to having the straight slope of the ‘Texan.’


This can vary from subtle to a very full breast
French

This is the most ‘natural’ of looks with a soft sloped curve from the chest wall to the breast mound.


It helps us to know what your ideal outcome in terms of shape would be. That of course does not always mean that it is achievable but we can work with you knowing your ideals and explaining what might and what might not be attainable and where we have to compromise. It is essential for us to understand the outcome you would not like to have. There are also some situations that an implant will not ‘fix:’
What won’t be changed by an implant alone:
Breast Droop:
The lower part of the breast will often drop after pregnancy and weight loss. An implant can fill out the volume but once all has settled the degree of droop will still be there.




If you want to address the droop then a ‘breast lift’ will be needed with or without implants, however you may not want scars. Occasionally we can compromise with a tall anatomical implant that fills out the bottom of the breast as well as the empty upper breast, avoiding the ‘tennis ball in a sock’ look that can happen if we use a round implant.


A round implant used in breast droop, sitting low on the chest wall. If used a tall anatomical implant would have filled in the upper chest hollow and given a nicer result.
The nipple position on the breast:
If your nipple is towards the bottom of the breast then it is not going to change without being surgically moved, however a compromise may be acceptable to you rather than having the scars of a lift. Again, using an anatomical implant can help by ’kicking up the nipple’ a little.





Tall anatomical implant used to help ‘kick up’ the nipple


If the nipples are lying to the outside of the breast, occasionally a shaped implant can be used to fill out the outside of the breast more. If the nipples are pointing inwards or outwards however, there is a risk that this can be exaggerated if a large augmentation is chosen, and it is often better to compromise on size.
The Cleavage area:
The cleavage is most often determined by the shape of the underlying chest wall and the attachment of the ribs to the breast bone, and how they slope away from the breast bone. If the natural cleavage is wide it is tempting to place the implants closer together, but this means that the inner edge of the implants will only be covered by skin and become visible. If the natural cleavage is wide then high, round implants will emphasize this, giving a railroad look between the breasts. This effect can be softened by using anatomical implants. A narrow cleavage can become a cleft if higher profile round implants are used.
 Narrow cleavage
Narrow cleavage

 Wide cleavage
Wide cleavage
Surgical Techniques
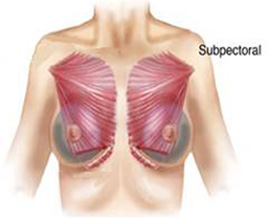
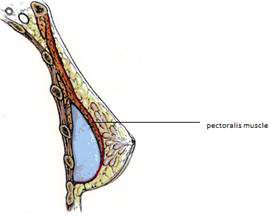
Subpectoral:
The implant is placed under the pectoralis muscle which runs from the upper ribs and breast bone across the front of the shoulder joint to the upper arm. This muscle is strong and used in upper chest work such as in swimming, push ups etc. The benefit of going ‘under the muscle’ is that it can smooth over the upper edge of the implant avoiding the ‘speed hump’ effect which can be obvious in a high profile round implant, or if you are very thin. A guide is if you can pinch less than 1.5cm thickness of fat where the top of the implant will sit then you may need the implant to be placed under the muscle if a round implant is used.
A downside of placement under the pectoralis muscle is that the lower inner attachment of the muscle needs to be separated off the ribs and breast bone for the implant to lie in the correct position. This is more painful in recovery. If you do a lot of upper body exercise then there is a chance that the muscle activity will push the implant outwards, widening the cleavage in time, and also the muscle activity might become visible through the skin creating a crease across the breast.

 Round subpectoral mod profile
Round subpectoral mod profile

 Round subpectoral high profile
Round subpectoral high profile

 Subpectoral anatomical
Subpectoral anatomical
Subglandular:
The implant is put beneath the breast gland in front of the muscle. This has an advantage in that the lower breast can be reshaped with some spreading of the tissue, to widen the base or lift the nipple a little. This technique also yields a faster recovery time than if the implant is placed underneath the muscle.

 Round subglandular implant
Round subglandular implant
Subfascial:
This is a technique which confers some of the benefits of ‘under the muscle’ without having to cut the muscle. The implant is placed under the fibrous outer layer of the muscle and so smooths over the top of the implant.

 Round subfascial implants
Round subfascial implants

 Anatomical subfascial implants
Anatomical subfascial implants

 Anatomical subfascial implants
Anatomical subfascial implants

 Anatomical subfascial implants
Anatomical subfascial implants
Dual Plane:
This is combination of techniques in which the top of the implant is ‘under the muscle’ and the lower part is over the muscle. This technique is good in women who are relatively thin and have breast fed to help lift the nipple slightly.

 Dual plane round implants
Dual plane round implants
The Incision
The surgical access can be from underneath the breast, the armpit or around the nipple. There are pros and cons to each and again the choice will be made together.
Implants
There is a huge range of implants available in different shapes and sizes. It used to be that you would choose a round implant of a certain size and that would make the breast that you have bigger, but not have much effect on shape. This is still an approach that is popular and one that you will see on the internet on many sites. Cohesive gels have meant that an implant can be selected in order to influence shape change, and so we can be a lot cleverer in obtaining a better outcome for you.
Most patients are suitable for round implants, saline or gel, but there are occasions when an anatomical implant can be advantageous. If you want a youthful round top this can be achieved with a high profile round implant underneath the muscle, or the same effect can be achieved by using a thicker anatomical implant in front of the muscle.


 Low, moderate and high profile round implants
Low, moderate and high profile round implants



 Different shaped anatomical implants with different thicknesses
Different shaped anatomical implants with different thicknesses
An anatomical implant can lift the nipple if your breast is a little droopy after breast feeding. If your chest is long with your breasts sitting low this can be disguised with a tall anatomical implant. If your ribs slope down and out, a wide U cleavage can be avoided with anatomical implants. They also work well in athletes with well developed pectoral muscles.
The outside coating of the implant is normally silicone and can be textured or smooth; however there are alternative texturings also available, such as polyurethane. Implants are filled with either saline or a cohesive silicone gel. There are differences in the amount of fill and how cohesive the gel is. These choices are determined a lot by the surgical approach chosen, the look you want and your tissues; also if you have had previous surgery. Dr Ngan will guide you through this at the consultation.
At the Aesthetic Breast Surgery Centre we work with you to try and achieve the results and look that you want, using our expertise and experience along with a range of surgical techniques and the wide array of implants available. To assist in our planning we use state-of the art 3D computer imaging software. As with all technology, it has limitations in that it does not show how your tissues will redrape over an implant, especially with time.
Important Issues to consider
Breast surgery as with all other surgery has its risks and complications. We all need to be prepared for when things do not work out as you hoped, and also to work together beforehand to minimise the risks. You need to be fully aware of these issues and know how we will address them, so that ultimately you can achieve a good result. When making your decision to go ahead with surgery, you need to be aware that your ideal may not be achievable and some compromises may need to be made. You need to be able to accept the risks and understand the following issues;
Capsules
This refers to the scar tissue around an implant. Whenever anything foreign is placed in the body, it becomes encased in scar tissue. Breast implants are no exception. Scar tissue can vary, and in some people it can thicken, harden and contract. This squeezes the implant so that it becomes more spherical and can ride up, giving rise to an unnatural round appearance. In a few people this can happen quite severely even within a matter of months. In others it can come on quite slowly over years and many patients will have no problem at all. Unfortunately we have no way of testing who is susceptible to this problem. Hardened, contracted capsules are one of the biggest problems associated with breast implants that we deal with.
There are a few factors that have been suggested to be linked with thicker capsular formation;
Collection of blood around the implant
Infection around the implant
Any radiotherapy to the breast
Factors that have been suggested to reduce the risk of capsular thickening;
When the implant is in front of the muscle, texturing of the implant shell has been shown by some studies to reduce this risk Placement of the implant behind the pectoralis muscle Avoiding any bacterial contamination as the implant is placed in the wound and incision selection Saline implants have a lower risk than gel implants
This capsule does in fact provide some protection. In women with the old type ‘runny’ silicone gel implants the shells were often thin and with time have ruptured. The gel is contained within this capsule and even though in some patients the implants may have ruptured some time ago the patient has been unaware of this fact as they have not caused any problems. Remember capsule is scar tissue, and is not harmful to your health. However because it looks unsightly and feels uncomfortable you may want it treated.
Mammography
The breast implant is placed behind the breast which spreads out over the surface of the implant. This makes standard mammography trickier to perform. In Australia augmented breasts undergo a displacement technique mammography examination, sometimes followed by an ultrasound and a physical examination. Radiographers are specially trained to deal with breast implants so that the chances of missing an early cancer are minimal as are the chances of damaging an implant. One in ten Australian women will develop breast cancer so regular mammograms are vital. Once you are over forty years of age you will need to make an appointment with Breast Screen telling them that you have breast implants so that they can arrange for you to have a proper assessment. Self examination is possibly easier with an implant, as all the breast tissue is spread over the implant, so making it thinner and easier to feel any changes. There are many studies which show that breast implants DO NOT increase the risk of developing breast cancer.
How long do implants last?
Nobody knows the answer to this question. Implants stay in until there is a problem. There is no set time span attached to them and to have them changed means further surgery and a general anaesthetic. The majority of patients with breast implants will need further surgery at some stage, either for correction of capsules or changes in breast shape. It is important to consider the future financial implications of this when deciding on having a breast augmentation. It is reasonable to expect that the shearing forces on an implant will cause the implant shell to weaken and eventually rupture. The only reliable test to look at the integrity of an implant is an MRI examination, which is unfortunately not fully covered by Medicare so there will be an out of pocket component to pay. The US FDA is recommending a MRI at five years and every two years from then on. Again one must consider the long term cost implications of this when considering an augmentation.
Anatomical implants will last an average of fifteen years, and round implants on average will last approximately ten years. High Cohesive Gel 100% round fill implants are thought to have a similar longevity to Anatomical implants.
Very rarely as implants wear out tiny amounts of silicone can be transported through the capsule and cause lumps in the breast or armpit. These are very easily distinguished from cancer when tested and do not make you ill. They are an indication that the implants are wearing out and need to be replaced.
Breast Feeding and Pregnancy
Most women can breast feed successfully after breast implant surgery. There have been many studies investigating the ability to breast feed after breast augmentation, and all have failed to show any problems with feeding a baby, regardless of whether the implants are gel or saline.
The effects of pregnancy and feeding on your breasts still occur. After children the breasts may shrink back to a softer version of what they were. Sometimes the breasts do not shrink back completely and you may consider a tightening of this loose skin or very occasionally replacement of your implants with bigger ones if the volume of your breasts has reduced.
Implant deflation
With time the breast implant shell weakens and in a saline implant this may lead to a deflation. The saline is harmless and rapidly absorbed. Obviously in this event another operation is required to replace the implant.
Feel and Visibility
Gel implants feel the softest and most natural. Anatomical implants are filled with a more solid gel to maintain the shape and so feel thicker. Saline implants can feel like a thick plastic bag filled with water when palpated through the skin. Occasionally patients have reported the sensation of sloshing of the saline. The folds in saline implants are much more of a problem than with gel implants, and these can be visible especially in thin patients. To reduce the visibility they need to be placed behind the pectoralis muscle, but this does not cover the lower outer part of the implant where ‘wrinkles’ may be seen.
The edges of the implant may also be palpable or visible. This is usually hidden under the breast fold, and so is not a big problem. However in thin patients even the upper edge can be visible, and in this case it is often better to place the implant under the muscle. In thinner patients even the ripples of thick gel implants can sometimes be seen.
Infection
This can be disastrous. Most infections occur secondary to bacteria passing in the circulation, from another site such as a sore throat, a dental filling, an infected finger etc. Your implants, being foreign in the body, are a perfect environment for bacteria to multiply around especially in the first few weeks following surgery. If you do have a sore throat, dental problems or other infections then in the first two to three months we would recommend a course of antibiotics, even though you would not normally need them.
Depending on the severity of the infection intravenous antibiotics, ultrasound guided needling of the infection, surgical wash out, and ultimately removal of the implants with replacement three months later may all be required.
Bleeding
You may bleed after the operation, and if this occurs it will mean a return to theatre to stop the bleeding and wash out the implants.
Wound healing
Rarely the wound comes undone and needs restitching. Sometimes a more extensive repair may be required. There is a high risk of infection in this situation. This is more likely to occur with larger implants and in smokers.
Scarring
Troublesome scars are rare in breast augmentation surgery but every scar has the potential to become thick and red. Nearly all scars will fade out given sufficient time (years) apart from a very few which are true keloids. You must bear this in mind when deciding on incision site placement.
Sensitivity and numbness
It is not unusual for an area of the skin near the incision to be numb after the operation, and this nearly always recovers. The nipple sensation may also alter and the nipples may be numb. In almost all cases this will recover within a few months, but there is a small risk of permanent loss of sensation. Occasionally the nipples can become over sensitive, but with desensitisation will settle down.
Cosmetic Satisfaction
It is not always possible to achieve your desired cosmetic outcome and there is always the chance that you could be disappointed. To get your breasts perfectly even is virtually impossible. We all have some degree of asymmetry, and this can become more obvious after surgery. Very occasionally the implants can settle to an uneven position and may need a surgical revision.
Human Adjuvant Disease and other health scares
This is a name that was given to a collection of symptoms including weight loss, joint pains, and fevers in women that had silicone breast implants. No other cause was found for their problems. With this concern about a potential major health risk, silicone breast implants were withdrawn from use in breast augmentation until full scientific studies were completed. An editorial in the New England Journal of Medicine summarized the findings. This disease entity is as prevalent in women without breast implants as those with, and thus no causative link can be made. The Therapeutic Goods Administration (TGA) has now allowed silicone breast implants back on the market.
There are always going to be ongoing investigations as to possible health risks associated with implants and you will hear of them from time to time. It is important you keep up your annual check-ups so that we can keep you updated on any relevant issues.
Potential Link with Lymphoma
There have been a few incidents of a rare type of blood cancer starting in the breast of women who have breast implants, and this is under international investigation as to whether there is a true link or if this is a coincidental link.
This is the statement put out by the TGA in Australia on their website:
Report of lymphoma associated with breast implants
27 January 2011
On 26 January 2011, the US Food and Drug Administration (FDA) announced a safety communication to warn about an association between breast implants and anaplastic large cell lymphoma. The risk of a patient developing this type of lymphoma is very low. The Therapeutic Goods Administration (TGA) has been monitoring the situation and has been in communication with the FDA and specialist groups over the past year on the issue. The Australian Society of Plastic Surgeons posted guidance for patients on this issue in March 2010.
Women with breast implants should continue to routinely monitor their breast implants and consult their implanting surgeon if they have any concerns. At this time, TGA does not recommend prophylactic breast implant removal in patients without symptoms or other abnormality.
Additional information
- Anaplastic large cell lymphoma (ALCL) is a rare cancer of the immune system that can occur anywhere in the body. According to the Surveillance, Epidemiology, and End Results Program of the U.S. National Cancer Institute, an estimated 1 in 500,000 women per year in the United States is diagnosed with ALCL.
- ALCL in the breast is even more rare; approximately 3 in 100 million women per year in the United States are diagnosed with ALCL in the breast.
- Although there are no equivalent data for Australia, the rate of ALCL is likely to be the same in Australia as in the US.
- An FDA review of the scientific literature published from 1997 through May 2010 identified 34 unique cases of ALCL in women with breast implants throughout the world. Four of these cases are from Australia.
- The 34 cases of ALCL in women with breast implants identified by the FDA is extremely small compared to the estimated 5 to 10 million women who have received breast implants worldwide.
- Nevertheless, based on these data, it is possible that women with breast implants may have a very small but increased risk of ALCL.
- Because the risk of ALCL appears very small, the TGA believes that the totality of the evidence presently available continues to support a reasonable assurance that approved breast implants are safe and effective when used as labelled.
- In total, FDA is aware of approximately 60 case reports of ALCL in women with breast implants worldwide. This number is difficult to verify because not all cases were published in the scientific literature and duplications may exist in the reporting.
- Patients with breast implants should continue to routinely monitor their implants in accordance with advice given to them by their implanting surgeon. If they notice any changes, they should contact their implanting surgeon to discuss their concerns.
- The FDA and the TGA will continue to evaluate the available information to understand the nature and possible factors contributing to ALCL in women with breast implants.
Anaesthetic Complications
Untoward anaesthetic events occur very rarely. They include allergies and anaphylaxis, deep vein thromboses, heart attacks, breathing problems, and awareness during the operation. This is why you have your procedure in hospital with a qualified anaesthetist and with full back-up facilities readily available.
The Consultation

For your first appointment you will need to allow about one hour. During this consultation Dr Ngan will examine your breasts and will discuss with you the different surgical techniques and implants available. Together you will work out what may and may not be achievable for you, and she will give you her recommendations. It is helpful if you can bring along photographs of what you like and what you don’t like to the consultation, so that she can have some understanding of your desires and can work out with you what is practically attainable. This process is aided by the use of secure, state-of the art Crisalix 3D imaging software, which produces graphic simulations of your potential appearance post-surgery.
Dr Ngan will also explain what complications are associated with breast augmentation, and how such an eventuality is dealt with. The potential long term problems of such a procedure are also discussed in detail. This assists you in making a fully informed decision. Any decision to undertake such a surgical procedure should not be taken lightly.
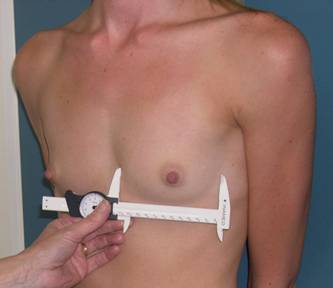
Implant Selection
It is important that the implant selected is appropriate not only in shape and size, but is a correct fit for your chest and tissues. Precise measurements of your chest wall and tissue thicknesses are taken. These measurements, along with an understanding of the desired shape and size of your outcome, are used to assist in making the selection. These measurements are also used in the 3D imaging program Crisalix, which provides a rough guide in showing you how you might look post-operatively. It is very important that you understand that everyone’s tissues are different, especially the way they will lie over an implant, however this imaging is helpful in providing an idea of how you will look. It is very helpful in demonstrating any chest wall variations that may influence your outcome. We also use ‘sizers’ and place them in a surgical bra to help you judge how you look. You can then discuss whether you would like to be bigger/smaller etc. Using these tools, we can together devise the right implant size and shape for you.




Following your consultation you will be given a written summary of what has been discussed. You will be provided with relevant pamphlets and a written estimate of costs. We encourage you to take this home and study it and write down any questions you may have.
Second Appointment
If you decide you would like to proceed with surgery then you will be offered a second appointment. You will see Dr Ngan again and have the opportunity to ask any further questions. You will be given relevant paperwork that is required. We encourage you to ask anything that you are unsure about, no matter how trivial it may seem. You are very welcome to come back just for another chat to further discuss the surgery. This does not mean that you have to go through with it!
The Operation

The surgery takes place in fully-accredited hospital. It is our belief that your safety is paramount concerning both surgery and anaesthesia. You will have the option of having your operation in Melbourne or Geelong. The procedure is performed under general anaesthesia, and a specialist anaesthetist will be giving the anaesthetic. You will be able to go home later that day. The operation takes about an hour, and at the end of the procedure local anaesthetic is used to minimize pain. You will be given a prescription for pain relief prior to leaving the hospital.
Post-Operative Care
If the implants are in front of the muscle recovery is normally within a week, however if the implant needs to be behind the muscle then you will be sore for a little longer, and can take up to 2 weeks to recover. Most patients can expect to be back at work within a week or two. We discuss with you the practical issues such as time off work, managing family etc. Due to the techniques used, the pain relief medication required is usually fairly simple, consisting of paracetamol and anti-inflammatories plus some stronger tablets ‘just in case’, but these are rarely needed.
The wounds are closed with absorbable stitches and paper tape. If you have anatomical implants your breasts will be taped up for ten days to prevent rotation. You can shower and dry the tapes with a hair dryer.
You will be seen within a few days of your operation to check on how you are doing and that the postoperative bra is fitting well. You will be seen again ten days to two weeks following the procedure and then as often as need be. You will be in a surgical bra for four weeks both day and night, followed by four weeks of wear during the day time only. If you have any concerns, please give us a call; we encourage you to come in and see us if you are worried about anything. Dr Ngan is on call day and night for any urgent concerns. Following these initial reviews, we usually see you at twelve weeks, six months and twelve months following the operation. You will then require an annual check up.
Exercise
You can go back to low impact exercise such as walking, bike riding, etc, but all high impact exercise and ‘bouncing’ including running should be avoided for at least six weeks. This allows scar tissue to form to support the implant and minimise the risk of it dropping. If your implant is under the muscle you should avoid heavy chest exercises.
Long Term Care
Breast implants do not last forever and they eventually wear out. Your body also changes with time and you may develop encapsulation (a build up of scar tissue around the implant). You will need further surgery at some stage to change the implants or address changes in your breast tissue. It is important that you understand that you need long term maintenance. We offer an annual check up of your breasts. Once you are over forty-five years of age it is important that you attend Breast Screen every two years for screening mammograms. There is no increase in the risk of breast cancer if you have implants, but one in ten women contract this disease and so screening for early detection is essential.
Once gel implants have been in for five years or more we offer an MRI scan every two years to look at the implant itself and check its integrity. The cost of ongoing maintenance of your implants is something that you need to consider carefully as part of your initial decision in having surgery.
Costs
You will receive a written quotation that fully explains the cost of the surgery. This includes post operative care, bras and dressings. Insurance companies do not usually give you any cover for this type of surgery but it would be worth checking with your health fund as they do occasionally contribute towards the hospital costs.
Disclaimer
All before and after photographs are of patients that have had surgery performed by Dr Ngan or Ms Corduff and have consented to their photographs being used. The photographs have not been altered. Results may vary from individual to individual.